

Полная версия
Polarity Analysis in Homeopathy:
The questionnaires for chronic illness also contain a free-format field at the beginning where patients can describe their chief symptoms, followed by a list of modalities and polar symptoms where patients underline those that match their illness. These are significantly more comprehensive than the checklists used for acute illness. In addition, important non-polar symptoms are listed. Along with the questionnaire for the chief symptom, the patients or children’s parents also receive a questionnaire for additional complaints, with which to register concurrent complaints of lesser importance. We used only the symptom formulations from PB when creating the checklists and questionnaires. In other words, these are repertory-specific. This procedure was chosen so that patients themselves can translate their symptoms into the language of the repertory. It is a potential source of error if the homeopath performs this step. Symptoms (rubrics) with fewer than ten assigned remedies are not used since, as individual symptoms, they unnecessarily restrict the choice of remedies, which can also lead to incorrect prescriptions.
The lists of currently available checklists and questionnaires are shown in tables 5 and 6. The complete checklists and questionnaires can be found in chapter 7, Tools. You can also download them from the author’s website (www.heinerfrei.ch). Chapters 2 to 5 describe in detail how to use them, and include many cases to clarify the method and to offer a sound practical grounding.
Patients – or the patient’s parents for children – download the checklists for acute illnesses directly from our website, fill them out while observing the symptoms and then bring them to the consultation – or if they have not already been completed when the patient arrives, they are filled out in the practice during the consultation.

Table 5: Checklists for Acute Illness
For chronic and multimorbid patients, the entire process of casetaking takes place on two separate dates. The first consultation includes the initial casetaking plus physical examination, with further tests scheduled as necessary, and finally a conventional medical diagnosis is made. Then the patients or parents receive the relevant questionnaires, which they prepare at home and bring back following an observation period lasting two to four weeks, so that the remedy can finally be chosen using all the information available.
When choosing the remedy, we evaluate the checklists and questionnaires, then discuss the symptoms given by the patients so that we can be sure that we have correctly understood the patient’s complaints, and what has been written down or underlined. We finish the casetaking by asking some supplementary questions.

Table 6: Questionnaires for Chronic Illness
1.5.2 REPERTORISATION
Boenninghausen’s PB is based on the idea that the valuable modalities, sensations, and findings of a remedy are capable of generalization. In other words, the modalities, sensations, or findings observed in clinical healing in various locations can be successfully transferred to other locations – that is, they can be generalised. This is the principle underlying the dissociated repertorisation, in which a complete symptom can be broken down into its elements and these can be repertorised individually. This means that a particular symptom restricts the choice of remedy less than with a synthetic repertorisation, in which the symptom is repertorised as a whole with all its elements. Synthetic repertorisation carries the risk that a case is restricted to one or a small number of remedies due to particular symptoms. When using a Kentian style of repertorisation in such cases, we often face the problem that not all symptoms can be assigned to a single remedy. The requirement that the remedy reflects the totality of symptoms is then no longer possible.
For our repertorisation, as already mentioned, at least five polar symptoms should be used if possible. If this number cannot be reached or if the polarity analysis is not sufficiently clear, further non-polar symptoms are used to differentiate the remedy. Table 7 shows the repertorisation scheme for polarity analysis. In theory repertorisation with PB could be performed manually using a corresponding table. Yet it is easier and faster to use computer software for this purpose. There are now at least four German Boenninghausen software packages with integrated polarity analysis,8,15,16,17 two of which are also available in English.8,16 In this book we use and explicitly recommend the program version V 2.6.0, 2012 of the Boenninghausen Arbeitsgemeinschaft.8 This has proved to be a simple, straightforward, and very reliable tool.
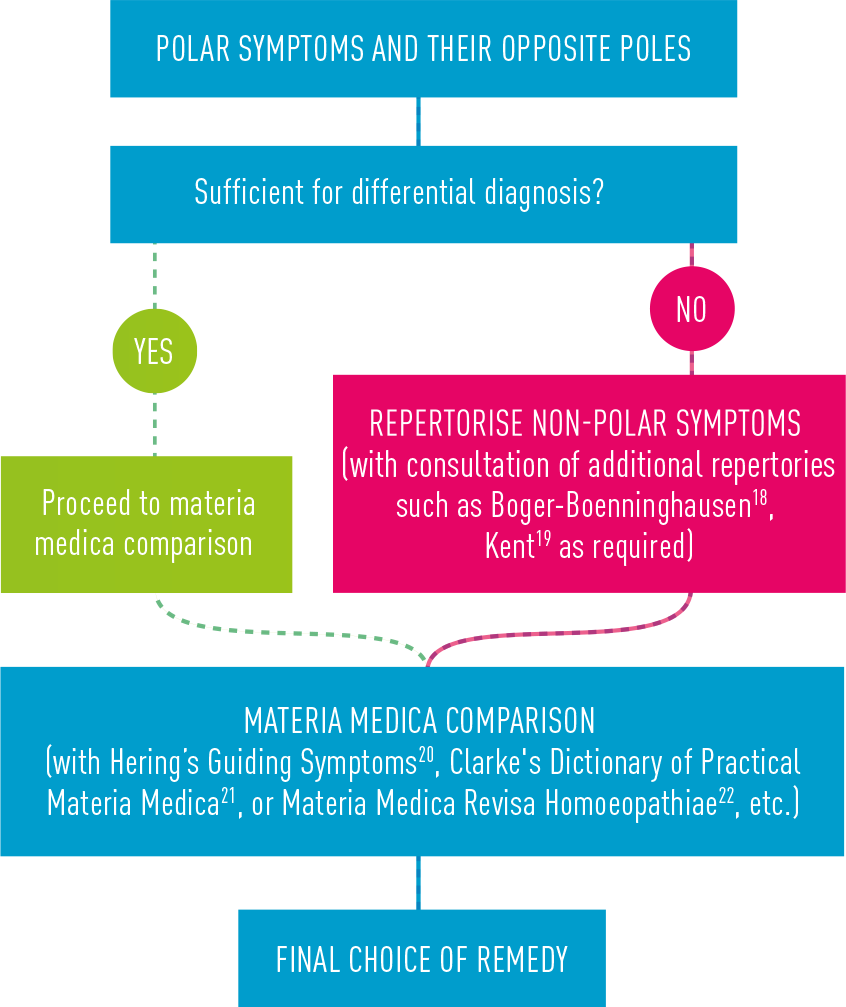
Table 7: Repertorisation Procedure for Polarity Analysis
We prefer this software because it is the only one that uses the revised edition of Boenninghausen’s PB7, containing his final insights into the grading of symptoms as well as numerous entries by him. It has the advantage of being very clearly laid out and easy to use. The good results of polarity analysis show that it has a so-far-unmatched level of reliability.
The most important criteria for the weighting of the repertorisation results are the absence of contraindications and the size of the polarity difference, followed by the completeness with which symptoms are covered, and finally the match established during the materia medica comparison (table 8). The importance of the absence of contraindications and the size of the polarity difference are practically identical – neither takes preference. If we receive very many polar symptoms, as usually occurs for multimorbid cases, the completeness of the symptom coverage has a significantly lower weight than polarity difference and contraindications. With rather symptom-poor acute illnesses, however, this criterion of symptom coverage becomes more important. In the recommended software, the result of the repertorisation can be sorted by number of hits (click top left on screen, second row) – which corresponds to the completeness of the symptom coverage – or by polarity difference (click top left on screen, fourth row). We recommend using both sort criteria to achieve a good overview of the likely remedies.
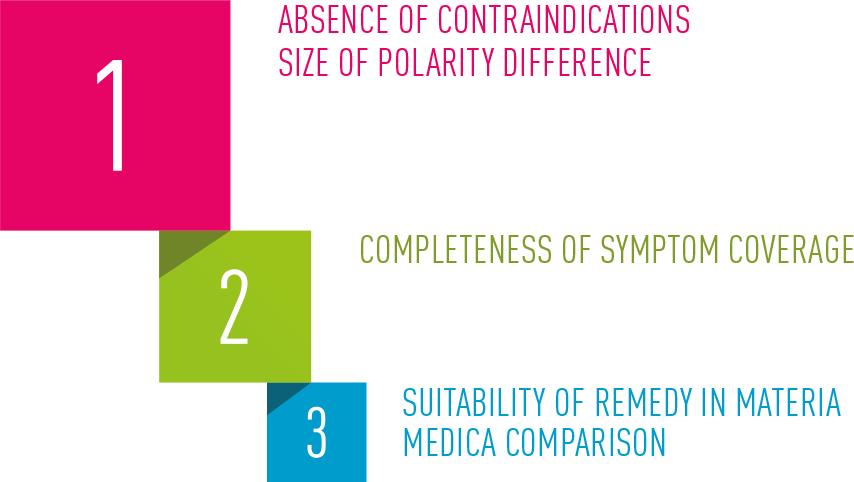
Table 8: Weighting of the Repertorisation Results
1.6 QUIZ 2: THE BOENNINGHAUSEN METHOD
7 List Boenninghausen’s hierarchy of symptoms (1st, 2nd, 3rd, 4th)!
8 What are the characteristics of a symptom?
9 Make a hierarchy of the reliability of the symptoms!
10 What do we today understand by pathognomonic symptoms? How was this term understood in the nineteenth century?
11 Define the genius of a remedy!
12 Define Boenninghausen’s grading of symptoms (1st, 2nd, 3rd, 4th, 5th grade)!
13 What did Boenninghausen mean by the term “contraindication”?
14 What is the essence of Hering’s Law and what role does this play when the patient has conflicting symptoms?
15 At what stage are the mind symptoms taken into account in the process of choosing a remedy?
> you can find the answers on p. 283/284
1.7 DOSAGE
The dosage of homeopathic remedies is a matter of individual preference. In tests with low potencies shaken by hand (5c, 7c, 9c, 12c), high potencies shaken by hand (30c and 200c), machine-made Korsakov potencies (1M, 10M, 50M, 100M) and Q potencies shaken by hand, I have formulated the following guidelines.
ACUTE ILLNESS
The most suitable remedy is administered in the potency 200 c as a single dose (two pellets). If the patient does not achieve an improvement of at least 50% within two days, the next best remedy – the “reserve” remedy, which was also given to the patient at the end of the consultation – is then administered, also in 200 c. With very acute illness or very severe pain, such as acute middle-ear infection, the time interval before administering the next remedy can be shortened to six hours to avoid the patient suffering for longer than necessary.
CHRONIC ILLNESS
The patient receives a dose of the most suitable remedy in the potency 200 c. The effect of the remedy is checked after four to six weeks or two months at the most. If the remedy has had the expected effect but the healing is not complete yet, or the effect is diminishing by the time of the check-up, further doses are administered in the potencies 1M, 10M, 50M, 100M, usually also with an interval of four to six weeks. In the complex casetaking study (CC = complex case, where the patient has three or more illnesses), presented in chapter 6, we have found that this procedure leads to the best course of improvement, in contrast to the practice of waiting until the improvement starts to diminish. With illnesses in which a strong initial aggravation is to be avoided (e.g. eczema), the first dose of the remedy can be administered in 30 c, since this is weaker and lasts a shorter time than 200 c.
Q POTENCIES
Liquid Q potencies are used in tricky therapeutic situations, such as patients with organ disease or with illness in which it is necessary to continue conventional medical treatment (for example, tumours). We generally start with Q3, administered over a period of four to six weeks, and then we switch to Q6 followed by Q9, and so on. The frequency of the dose depends on the type of illness. It can be daily or less often.
1.8 ASSESSING PROGRESS
Progress in acute illness can be assessed using the same criteria as those listed in section 1.7: if the patient achieves an improvement of at least 50% within two days, we wait; otherwise we administer the reserve remedy. Treatment is successful if the illness can be treated with the first or second remedy without any more consultations. Of course acute illness frequently resolves spontaneously. Healing can only safely be ascribed to the remedy in such cases when it occurs exceptionally quickly. For example, a meta-analysis by Del Mar and colleagues demonstrated that placebo treatment of acute middle -ear infection led to freedom from pain in 60% of patients within 24 hours.23 In contrast, a study with 230 patients suffering from acute otitis media showed that 39% of the children were pain-free six hours after receiving the first homeopathic remedy, and a further 33% of the children who received a second remedy were pain-free within 12 hours.24 Such improvements can be ascribed to the effect of the homeopathic treatment.
It is more straightforward to judge progress in chronic illness and multimorbid patients. We have found it useful to ask the patient to rate each complaint in terms of intensity and frequency on a scale of 1 to 10, where 10 is the worst state. This is done at the start of treatment and then at every check-up. In addition they judge their improvement, also on a scale of 1 to 10. This should ideally reflect the reduction in average symptom intensity. With the spreadsheet case log, presented in chapter 5, these patient assessments can be displayed in graphical form (see example below, figure 1).
Figure 1: Example of Graphical Progress Check (Ms D. T., 58 years old)
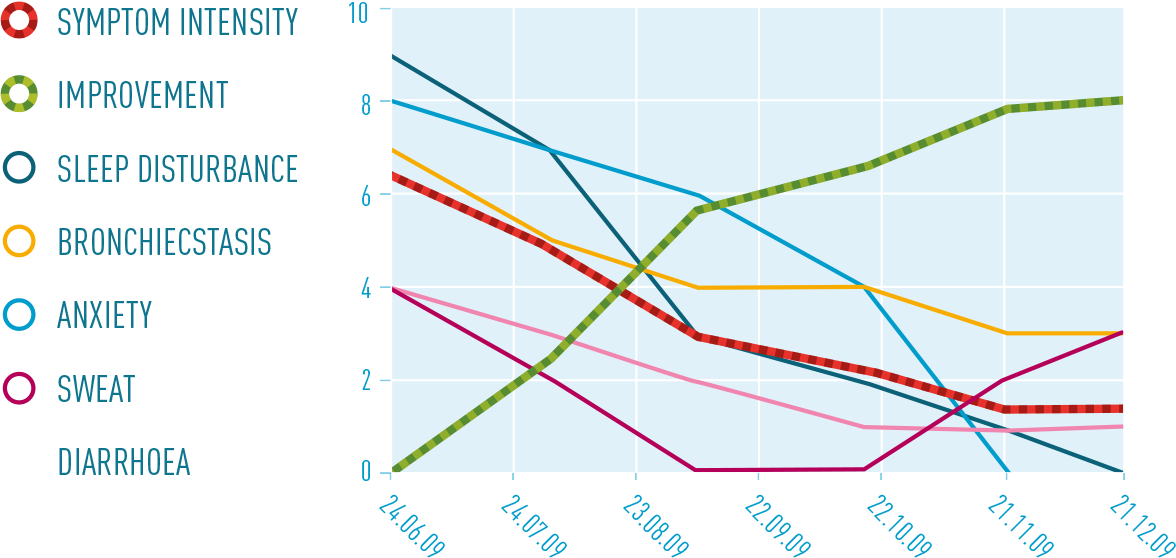
EXPLANATION OF FIGURE 1
The list of symptoms is displayed on the left and the progress of each symptom is displayed on the right. The red dotted line represents the average decline in intensity of all symptoms, while the green dotted line represents the global improvement subjectively experienced by the patient. All dates are DD.MM.YY.
1.9 PRACTICAL PROCEDURE
1.9.1 CASE 2: MS L.T., 44 YEARS OLD, ACUTE HEARING LOSS
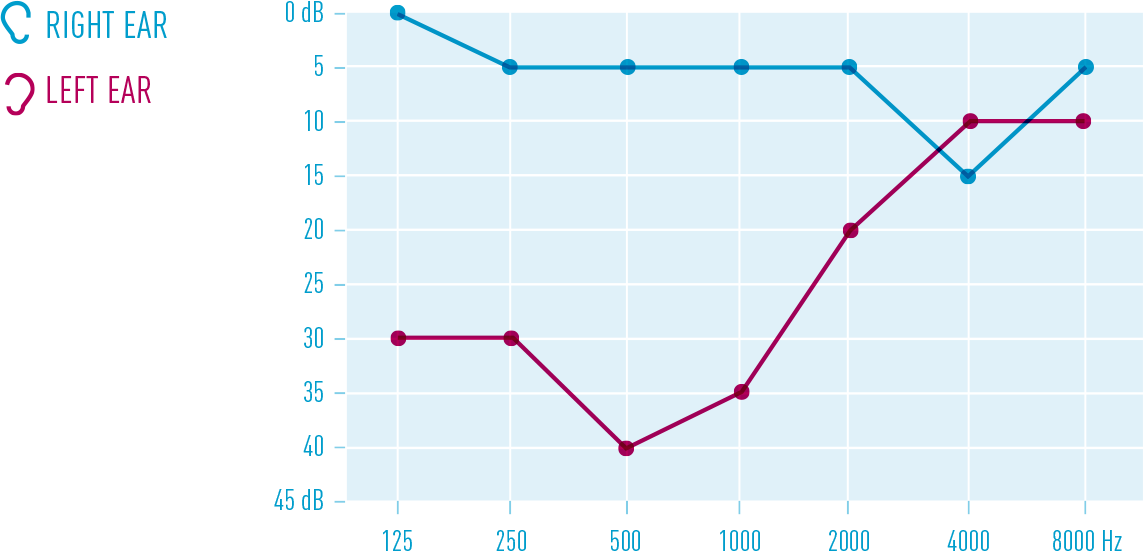
Ms T. is a highly industrious woman who, together with caring for her family of five, works 46 hours a week as a speech therapist. She comes for homeopathic treatment of acute hearing loss: while out riding the previous day, she suddenly felt a loud whistling in the left ear followed by severe ear pain and acute loss of hearing. Previous illnesses include atopy, migraine, and Raynaud’s phenomenon, which had practically disappeared during homeopathic treatment with Nux vomica in increasing potency. Due to mild arterial hypertension, she has been taking an angiotensin II receptor antagonist.* The examination reveals a normal eardrum and considerable loss of hearing on the left. Otherwise there are no pathological findings. After starting the homeopathic treatment, the patient is sent to the ENT physician for an objective diagnosis. The first audiogram shows low-frequency hearing loss (125-1000 Hz, figure 2). The right ear is normal.
Figure 2: Audiogram L.T. 24.11.08
He recommends treatment with a histamine agonist to improve blood circulation and a course of Prednisone (cortisone). The patient decides not to follow his advice. The choice of homeopathic remedy is shown below: following the initial investigation the patient is given the checklist for acute ENT and eye disease, with which she selects the following symptoms:
CHECKLIST FOR ACUTE ILLNESS

Date:__________________________ Patient name:_________________________
To enable us to find a suitable homeopathic remedy, we need you to precisely record here all changes in how you feel which have arisen during the current illness. To do this:
1) In the box below, write the main symptoms you have noticed with your illness:
MAIN SYMPTOMS Left ear: Noises whistling, ringing, Pain stabbing, pricking inward, Hard of hearing
_____________________________________________
2) Underline below whatever applies to you during your illness. For example: if it gets worse when you perspire, mark: during / after perspiration better / worse
OPEN AIR, WEATHER, TEMPERATURE, WRAPPING UP
• open air: better / worse • open air: desire for / aversion to • cold weather: better / worse • wet weather: better / worse • dry weather: better / worse • cold in general: better /worse • warmth in general: better / worse • when getting cold: better / worse • wrapping up warmly: better / worse • uncovering: better / worse • warm room: better / worse • during / after perspiration: better / worse • wet compress on body: better / worsePOSITION
• lying position: better / worse • lying on painful side: better / worse • sitting: better / worse • sitting bent over: better / worse • standing: better / worse • bending over: better / worse • muscles: flabby / tenseMOVEMENT, EXERCISE, REST
• movement: desire for / aversion to • movement: better / worse • walking: better / worse • stepping hard: better / worse • physical exercise: better / worse • mental effort: better / worse • resting: better / worseEATING, DRINKING, TALKING
• swallowing: better / worse • during / after eating: better / worse • cold food and drink: better / worse • after drinking: better / worse • cold water: better / worse • thirst: thirsty / absence of thirst • appetite: hunger / loss of appetite • saliva: more / less • talking: better / worseSLEEP
• after lying down: better / worse • while falling asleep: better / worse • during sleep: better / worse • while waking up: better / worse • while / after getting up: better / worseSIGHT
• light (bright): better / worse • darkness: better / worse • closing eyes: better / worse • pupils: dilated / contracted • reading: better / worse • looking at something close-up: better / worseSIDE
• side in general: left / right • inside of head: left / right • outside of head: left / right • face: left / right • eye: left / right • nose: left / right • ear: left / right • mouth: left / right • teeth: left / right • neck: left / rightSENSATION
• touch: better / worse • external pressure: better / worse • rubbing: better / worse