


Полная версия
Anatomy of bone system. The manual for medical students / Анатомия костной системы. Учебное пособие для медицинских вузов

Ничипорук Г. И., Гайворонская М. Г., Курцева А. А., Гайворонский И. В.
Anatomy of bone system. The manual for medical students / Анатомия костной системы. Учебное пособие для медицинских вузов
LIST OF ABBREVIATIONS
A., a. – arteria
Aa., aa. – arteriae
Art., art., – articulatio
Artt., artt., – articulationes
For., for. – foramen
Gl., gl. – glandula
Gll., gll. – glandulae
Lig., lig. – ligamentum
Ligg., ligg. – ligamenta
M., m. – musculus
Mm., mm. – musculi
N., n. – nervus
Nn., nn. – nervi
R., r. – ramus
Rr., rr. – rami
S., s. – sulcus
V., v. – vena
Vv., vv. – venae
PREFACE
Creation of the manual «Anatomy of Bone System» in English meets the requirements of modern Russian medicine and education. Nowadays, many English-speaking oversea students study in Medical Universities of Russia. Besides, many Russian school leavers have a good command of English, so they will be able to use this manual by taking into consideration the fact that many Russian medical specialists work abroad after graduating from the universities or take part in different international conferences and symposiums.
The English version of the manual is based on the Russian manual by professor I. V. Gaivoronskiy «Normal Human Anatomy» which has been published in Russia 9 times and is approved by the Ministry of education of Russia.
This manual introduces the main principles of the Russian Anatomy School, such as: detailed study of the general aspects and items of Anatomy including the development of organs and anomalies of the development. If we compare theoretical approaches to Anatomy in Russia and in other countries, we will see that our approach is based on the system descriptions of organs, i.e. we describe separately the Skeletal system, Articulations, Muscular system etc. Moreover, we use Latin terminology in describing the structure of organs, and discuss clinicoanatomical and functional problems. As for foreign manuals, many of them describe Anatomical systems in accordance with the regional and topographical principles.
The structure of our manual meets the requirements of modern standards of medical education in Russia which, in their turn, correspond to the major European standards. After each chapter, we give test questions and clinicoanatomical problems. The English and Latin terminology is given in accordance with the International Anatomical Nomenclature.
The authers srongly believe that the manual will allow future doctors to form the morphological foundation for the further study of theoretical and clinical disciplines. We also hope that it will be of great help to Anatomy teachers.
ПРЕДИСЛОВИЕ
Создание учебного пособия «Остеология» на английском языке является требованием современной системы медицинского образования в России. В настоящее время в медицинских университетах нашей страны обучаются студенты из различных регионов дальнего зарубежья. Кроме того, многие выпускники российских школ хорошо владеют английским языком, поэтому они так же смогут пользоваться данным пособием, принимая во внимание, что зачастую русские специалисты в медицине после окончания университета уезжают работать за рубеж или принимают участие в различных международных конференциях и симпозиумах.
Английская версия пособия базируется на учебнике профессора И. В. Гайворонского «Нормальная анатомия человека», который был издан в России 9 раз и имеет гриф Министерства образования Российской Федерации.
Данное пособие познакомит читателей с главными принципами Русской Анатомической Школы, которые заключаются в подробном изучении общих вопросов, в том числе развития органов и аномалий развития. В России преподавание анатомии ведется с функционально-клинических позиций и основано на описании органов по системам, т. е. отдельно изучается опорно-двигательная система, артросиндесмология, миология и другие системы. Также при описании строения органов акцентируется внимание на латинской терминологии. Что касается зарубежных руководств по анатомии человека, многие из них основываются на регионально-топографическом принципе без использования латинской терминологии.
Структура данного пособия соответствует современным стандартам медицинского образования в России, которые, в свою очередь, соответствуют важнейшим Европейским стандартам. После каждой главы мы приводим контрольные вопросы и ситуационные клинические задачи. Английская и латинская терминология приведена в соответствии с Международной анатомической номенклатурой.
Авторы выражают уверенность, что данное пособие позволит будущим докторам сформировать морфологический фундамент для последующего изучения теоретических и клинических дисциплин. Мы также надеемся, что оно принесет определенную пользу и преподавателям анатомии человека.
1. GENERAL ОSTEOLOGY
Osteology is the part of anatomy which studies bones. It is quite difficult to determine the exact number of bones, because their number changes with age. During life, more than 800 individual bony elements develop, 270 of them appear in the prenatal period, other ones appear after birth. The majority of individual bony elements fuse with each other, therefore the skeleton in an adult person contains only 206 bones (fig. 1.1). Apart from permanent bones, there may be inconstant (sesamoid) bones in mature age, their appearance is caused by specific features of the body structure and function.
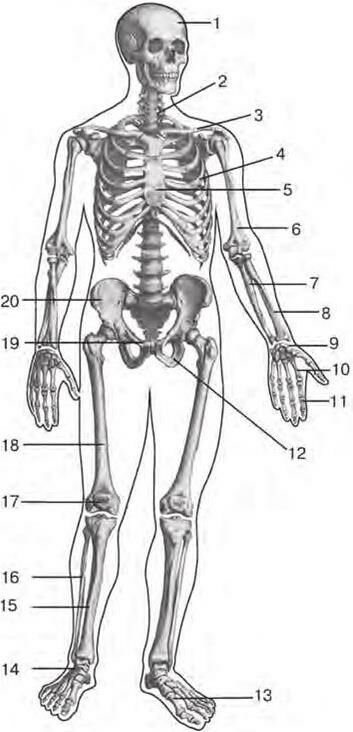
Fig. 1.1. Human skeleton (frontal aspect):
1 – skull (cranium); 2 – vertebral column (columna vertebrale); 3 – clavicle (clavicula); 4 – IV rib (costa IV); 5 – sternum (sternum); 6 – humerus (humerus); 7 – ulna (ulna); 8 – radius (radius); 9 – carpal bones (ossa carpi); 10 – metacarpal bones (ossa metacarpi); 11 – phalanges of hand (ossa digitorum manus); 12 – ischium (os ischium); 13 – metatarsal bones (ossa metatarsi); 14 – tarsal bones (ossa tarsi); 15 – tibia (tibia); 16 – fibula (fibula); 17 – patella (patella); 18 – femur (femur); 19 – pubis (os pubis); 20 – ilium (os ilium)
The bones, together with their joints, form the skeleton of the human body. It serves as a place for start and attachment of muscles, provides protection of visceral organs and also carries out the formbuilding and some other major functions.
1.1. Bone as an Organ
Bone, os, is an organ, which is a component of the musculoskeletal system. It hаs a typical form and structure, specific architectonics of vessels and nerves, it is constructed mainly from osseous tissue covered with periosteum on the outside; periosteum containing inside bone marrow, medulla osseum.
Each bone has a certain shape, size and location in the human body. The conditions of bone development and functional loads which bones are subjected to in ontogenesis influence the morphogenesis of bones. Each bone has a certain number of blood supply sources (arteries), which have specific extra- and intraorganic architectonics. Nervous structures of bones also have such features.
The bone is coated with periosteum on the outside, except the surfaces and places where articular cartilages are locted, and where muscles, tendons and ligaments are attached to the bone. The periosteum separates the bone from its surrounding tissues. It is a thin sheath of dense connective tissue which contains blood and lymphatic vessels and nerves. The nerves penetrate into the bone tissue from the periosteum.
The periosteum, periosteum, plays a major role in bone growth at thickness and in its nutrition. The osseous tissue is formed in the inner osteogenic layer of the periosteum. A bone lacking periosteum becomes inviable and necrotizes. The periosteum has a rich nerve supply, therefore it is very sensitive. During surgical operations, doctors try to maximally preserve the periosteum because of its very important role in reparative processes.
Almost all bones (except for most of the skull bones) have articular surfaces for junction with other bones. The articular surfaces are covered not with periosteum, but with articular cartilage, cartilago articularis. The articular cartilage has a specific, nonuniform structure: its superficial layer resembles a hyaline cartilage, the deep layer is fibrous.
The majority of bones have bone marrow inside – in spaces between lamellae of the spongy bone or in the medullary cavity, cavitas medullaris. The medullary cavity is covered inside with a specific sheath which is termed endosteum – endosteum. The endosteum, as well as the periosteum, plays a great role in metabolic processes in bones.
Bones of fetuses and newborns contain only red (haematogenic) bone marrow, medulla ossea rubra. It is a homogenous red color mass, rich in reticulate tissue, blood corpuscles and blood vessels. The total amount of red bone marrow is about 1500 cm3. In an adult, red bone marrow is partially substituted with yellow bone marrow, medulla osseum flava, which is mainly composed of adipose cells. Red bone marrow is substituted with yellow bone marrow only within medullar cavities.
1.2. Classification of Bones
It should be noted that there is no comprehensive classification of bones so far. For this purpose, various criteria are used in most of manuals on anatomy. At the same time, the principles of development and external structure features are often missed. Such feature as the structure of bones has an important clinical value. It determines the level of bone durability and specifications for treatment of injuries. In terms of phylogenesis, taking into consideration the existence of acranial and cranial organisms during the evolution, it is appropriate to divide bones into two groups: 1) bones of trunk and limbs; 2) skull bones. These bones differ from each other not only in their development but also in their structure.
According to the form and structure, four types of trunk and limb bones are distinguished: tubular, flat, volumetric and mixed bones.
Tubular bones have a cavity inside. They may be divided into long (humeral, forearm bones, femoral, leg bones, clavicle) and short (carpals, metatarsals, phalanges) bones.
In long tubular bones, one size prevails over other sizes. The middle part – diaphysis, diaphysis, (or body, corpus) of such bone has a cylindrical or triangular shape and consists of compact tissue, substantia compacta. Within the diaphysis, the medullary cavity is located. The bone ends – epiphyses, epiphyses, – are somewhat thickened. Their surfaces intended for joining with adjacent bones are covered with articular cartilage. On the inside, the epiphysises consist of spongy bone – substantia spongiosa, and on the outside there is a thin layer of compact bone – substantia compacta. Long tubular bones form the proximal and middle parts of the limb skeleton and play the role of leverages actuated by muscles. Short tubular bones form the distal parts of the limb skeleton and also consist of the middle part – the corpus and two ends called basis and caput.
Flat bones mainly consist of homogenous mass of spongy bone covered outside with a thin layer of compact bone. In flat bones, two sizes (width and length) prevail over 1.3. thickness. Such bones form the walls of cavities enclosing important organs, or represent extensive surfaces for attachment of muscles. Here belong the pelvic bones, sternum, scapulae and ribs.
Volumetric bones have the same structure, as the flat bones, i.e. they consist of a thin layer of compact bone outside and spongy bone inside. By shape, they resemble a cube with all dimensions roughly the same. Such bones are the carpal and tarsal bones. These bones are situated on the border between the middle and distal parts of the limbs, where not only high durability, but also high mobility is necessary.
Mixed bones are specific and complicated in shape. In their composition there are structural elements of volumetric and flat bones (vertebrae, sacrum, coccyx). Spongy tissue is contained in the bodies of these bones, and their other parts are mainly formed of compact bone. Such bones possess specific durability at continious loads.
Skull bones are classified by their location, development and structure.
According to location, they are divided into neurocranium bones and viscerocranium bones. According to development: into primary (endesmal), secondary (enchondral) and also mixed bones. The bones of the calvaria and viscerocranium are primary; the bones of the skull base are secondary; the occipital, sphenoidal and temporal bones are mixed; for example, the pyramid of the temporal bone and its mastoid part are secondary, but the squamous and tympanic parts of this bone are primary.
The skull bones have a very complicated external shape, thus it is appropriate to take their structure into consideration. According to the structure, it is possible to distinguish three types of the skull bones: 1) bones having diploё in their composition – diploic bones (parietal, occipital, frontal bones, mandible); 2) bones containing air cavities – pneumatized bones (temporal, sphenoid, ethmoid, frontal bones and maxilla); 3) bones built mainly from compact tissue – compact bones (lacrimal, zygomatic, palatine, nasal bones, inferior nasal concha, vomer, hyoid bone)The diploic substance is like spongy tissue, but its spaces between the osteal trabeculae are significantly smaller in diameter and have rounded shape.
1.3. Internal Structure of Bones
The internal structure of bones essentially differs in a fetus and in a newborn child. Therefore two types of osseous tissue are distinguished – reticulofibrous and lamellar. The reticulofibrous bone tissue is the basis of the embrional human skeleton. Its bony matrix is not arranged structurally, the bundles of collagen fibers are located in different directions, and they are directly connected with connective tissue surrounding the bone.
After birth, reticulofibrous tissue is replaced with lamellar tissue formed of osteal lamellae 4,5 – 11 mkm thick. There are osteal cells (osteocytes) in the smallest cavities (lacunae) between osteal lamellae. Collagen fibers in the bone lamellae are strictly arranged parallelly to their surfaces. They lose connection with the connective tissue surrounding the bone. They are connected with the periosteum only due to perforating (Sharpey`s) fibers running from the periosteum to the superficial layers of the bone. The lamellar bone is much more solid than the reticulofibrous bone. Substitution of one osseous tissue with another is caused by the influence of functional loads on the skeleton. On the section of a macerated bone (bone deprived of soft tissues), it is possible to see two types of the osseous tissue: compact and spongy. The compact bone, substantia compacta, is a solid bony mass located on the exterior of the bone. The osteal lamellae of the compact bone are very close to each other. The compact tissue coats the epiphyses of tubular and flat bones as a thin sheath. The diaphyses of tubular bones entirely consist of compact bone.
Spongy bone, substantia spongiosa, is formed by loosely located osteal lamellae. In the spaces between them there is red bone marrow. Spongy tissue forms epiphyses of tubular bones, bodies of vertebrae, ribs, sternum, pelvic bones and some hand and foot bones. Only the superficial cortical layer of such bones is comprised of the compact tissue. The spongy tissue of the skull bones has significantly smaller regularly shaped spaces in comparison with the trunk and limb bones. It has a specific name – diploё.
The structural and functional unit of the bone is osteon or Haversian system. It is possible to see osteons on thin sections or on histological preparations. The osteon is formed of concentrically arranged osteal (Haversian) lamellae which surround the Haversian canal in the form of cylinders of various sizes nested into each other. The Haversian canal contains blood vessels and nerves. The majority of osteons are oriented parallelly to the axis of the bone joining with each other in many points. The number of osteons is individual for each bone. For example, in the femoral bone this number is 1,8 per 1 mm2. Meanwhile, the share of the Haversian canal is 0,2 – 0,3 mm2. Between the osteons there are insert or intermediate lamellae which run in all directions. The intermediate lamellae are the remnants of destroyed old osteons. Processes of new formation and destruction of osteons continuously occur in bones.
There is a layer of internal circumferential lamellae, lamina circumferentialis interna in tubular bones on the border with the medullary cavity. They are permeated with numerous canals widening to spaces. Several layers of general (or external) circumferential lamellae, lamina circumferentialis externa, surround the bone on the outside. The perforating canals (Volcmann`s canals) containing blood vessels with the same name pass through them.
There are three types of osteal lamellae in the diaphyses of tubular bones: Haversian, intermediate and general (external and internal). The lamellae lie close to each other, they are located parallelly to the axis of the bone and form quite a thick layer of only compact bone. It is 1,5 – 5 mm thick. Thus the diahysis of a long tubular bone is a hollow cylinder with walls formed of compact bone. The cavity of this cylinder is termed medullary canal. The latter is connected with spaces of the spongy tissue in the epiphyses of the bone. The Haversian lamellae form the basic mass of compact bone, thus making up osteons. The intermediate lamellae fill in the gaps between osteons. External and internal general (circumferential) lamellae form the most outer and the most inner layers of the compact bone, being located parallelly to the bone surface under the periosteum and endosteum respectively.
The epyphises of tubular bones consist of spongy tissue which is also formed of osteal lamellae. In structure, spongy bone may have large and small spaces. There are red bone marrow and vessels in these spaces. Compact bone covers epiphyses only on the outside with a comparatively thin layer. Flat and volumetric bones have a similar structure. Lamellae of spongy substance are strictly arranged in each bone. Their direction coincides with that of the maximum compression and stretching forces. The environment of each bone determines its structure. Trabeculae form an integral system in several adjacent bones, which characterizes the trabeculae’s architectonics. Such structure of bones preconditions their maximum solidity. In vertebrae, the stretching and compression forces are perpendicular to the superior and inferior surfaces of the vertebral bodies. This corresponds to the fact that the trabeculae have mainly vertical direction in spongy substance (fig. 1.2). In the proximal epiphysis of the femoral bone there are arch-shaped systems of trabeculae which transfer pressure from the surface of the bone head to the walls of the diaphysis. Besides, there are trabeculae transfering the traction force of muscles attached to the greater trochanter (fig. 1.3).
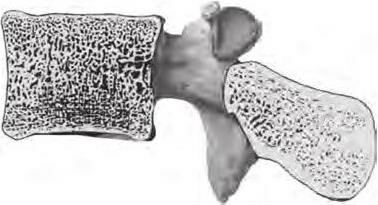
Fig. 1.2. Orientation of trabeculae in the vertebral body (saggital section)

Fig. 1.3. Orientation of trabeculae in proximal epiphyses of tubular bones: a – in femur; b – in tibia
Trabeculae running in the radial direction are typical of the calcaneus. They distribute loads equally over the surface of the calcaneal tuberosity which serves as a foot support (fig. 1.4).

Fig. 1.4. Orientaton of trabeculae in calcaneus
Compact bone is formed in places of the highest concentration of force trajectories. It is clearly visible on the section of the femoral, tibial and calcaneal bones where the compact tissue is thickened in the areas of crossing between force lines and the bone surface. Thus we can say that compact bone is the result of compression of spongy bone, and vice versa, it is possible to consider spongy bone as sparse compact bone. It should be noted that if static and dynamic conditions are changed (increase or decrease in functional loads), the spongy bone architectonics changes too, a part of trabeculae disappear, or new systems of osteal trabeculae develop. The spongy bone structure changes in a special visible manner after fractures.
1.4. External Structure of Bones
While describing the external structure of bones, we should pay attention to the surfaces, facies, of the bones, which may be flat, concave or convex, smooth or rough. Articular surfaces facies articularis, involved in formation of joints, are the most smoothly polished ones. In some bones the end is rounded, forming a head – caput; at the same time, the end of other bones has concavity, called articular fossa, or fossa articularis. The head may be separated from the bone body with a constricted part – neck, collum. If the articular end is extensive but slightly curved surface, it is termed condyle, condilus. The processes located near the condyle are named epicondyles, epicondyli, they serve for attachment of tendons and ligaments (they may also be called apophyses).
The following surfaces are distinguished in bones (depending on theirlocation in the human body): internal or external, medial or lateral etc. The surfaces are separated by borders, margo. The borders, in turn, are known as superior or inferior, medial or lateral etc. They may be smooth or serrated, blunt or sharp, sometimes they have notches, incisurae, of different sizes.
On the surfaces of bones, there may be such formations as: processes, eminences, depressions, openings etc. (bone process, processus; elevation, eminence, eminentia; large rounded elevation or tuberosity, tuberositas; hillock, tuber; bulge, protuberance, protuberantia; tubercle, tuberculum; sharp process – spine, spina; crest, crista; hollow in the bone, fossa; pit, foveola; groove, sulcus, opening, foramen; canal, canalis; small canal, canaliculus; fissure, fissura; cavity, cavitas).
1.5. Chemical Сomposition of Bone and its Properties
The chemical composition of a bone depends on the condition of the bone under examination, its age and individual characteristics. In a grown-up, a fresh bone which is not treated contains: water – 50 %; fat – 16 %; other organic substances – 12 % and inorganic substances – 22 %. A dehydrated and defatted bone contains approximately two-thirds of inorganic substances and one third of organic substances.
The inorganic substances are mainly represented by calcium salts in the form of submicroscopic crystals of hydroxyapatite. The microscopic examination shows that the axes of crystals are oriented parallelly to osteal fibers. The crystals of hydroxyapatite form mineral fibers.
The organic substance of the bone is called ossein. This protein is the type of collagen. It forms the basic substance of the bone. Ossein is contained in osteal cells – osteocytes. There are osteal fibers containing protein – collagen – in the intercellular matrix of the bone. When bones are boiled, the proteins (collagen and ossein) form glutinous mass. It should be noted that the bony matrix contains mineral fibers, apart from collagen ones. The interlacement of organic and inorganic fibers determines the specific features of osseous tissue: durability and elasticity.
If a bone is treated by acid (decalcification), the mineral salts are removed. Such bone, containing only organic substance keeps its shape in all details, but becomes much more flexible and elastic. If the organic substance is removed from the bone through burning, the elasticity is lost. Such bone is very fragile.

