 полная версия
полная версияMedieval Medicine
The other great French surgeon of the fourteenth century was Guy de Chauliac, who well deserves the name of father of modern surgery. He was educated in a little town in the South of France, made his medical studies at Montpellier, and then went on a journey of hundreds of miles to Italy in order to make his postgraduate studies. While it is not generally realized, for some seven centuries before the nineteenth Italy was the home of graduate teaching in all departments. Whenever a man in any country in Europe, from the beginning of the twelfth until the end of the eighteenth century, wanted to secure opportunities for the higher education that were not available in his home country, he went down into Italy. At the beginning of the nineteenth century France usurped Italy’s place for half a century, and Germany pre-empted the position to a great degree during the latter half of the nineteenth. The journey to Italy in the Middle Ages was more difficult, and involved more expense and time, than would even the voyage from America to Europe in our time; yet many a student from France, Germany, and England made it for the sake of the postgraduate opportunities, and it is matter for professional pride that this was particularly true of our medieval colleagues in medicine and surgery.
Larger Image
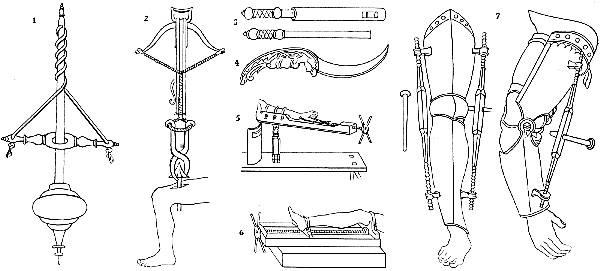
SURGICAL INSTRUMENTS OF GUY DE CHAULIAC, NOS. 1, 2, 3, AND 4 (FOURTEENTH CENTURY);
AND SURGICAL APPARATUS OF HANS VON GERSSDORFF, NOS. 5, 6 AND 7 (FIFTEENTH CENTURY)
After plates in Gurlt’s “Geschichte der Chirurgie”
To know Guy de Chauliac’s works well is to have ready contradictions at hand to practically all of the objections so frequently repeated as to the lack of scholarly work during the Middle Ages. For instance, Guy de Chauliac insisted on the value of experience rather than authority, and of original work rather than mere copying. He criticized in bitter satire John of Gaddesden’s book on medicine, called after the fashion of the time by the poetical title “Rosa Anglica,” of which he said: “Last of all bloomed the scentless Rose of England, which on its being sent to me I hoped to find bearing the odour of sweet originality. But instead of that I encountered only the fictions of Hispanus, of Gilbert, and of Theodoric.” His mode of satirical expression is all the more interesting and significant, because it shows that the men of the time were critically minded enough as regards many of the passages in the writings of their predecessors with which fault has been found in the modern time, though we have usually been inclined to think that medieval readers accepted them quite uncritically. Chauliac’s bitterest reproach for many of his predecessors was that “they follow one another like cranes, whether for love or fear I cannot say.”
Chauliac’s description of the methods of anæsthesia practised by the surgeons of his time, especially in cases of amputation, is particularly interesting to us because the anæsthetic was administered by inhalation. Chauliac says:
“Some surgeons prescribe medicaments, such as opium, the juice of the morel, hyoscyamus, mandrake, ivy, hemlock, lettuce, which send the patient to sleep, so that the incision may not be felt. A new sponge is soaked by them in the juice of these and left to dry in the sun; when they have need of it they put this sponge into warm water, and then hold it under the nostrils of the patient until he goes to sleep. Then they perform the operation.”10
Chauliac was particularly interested in the radical cure of hernia, and he discusses six different operations for this purpose. Gurlt points out that Chauliac’s criticism of these operations is quite modern in its viewpoint. He declared that practically the object of radical operations for hernia is to produce a strong, firm tissue support over the ring through which the cord passes, so that the intestines cannot descend through it. It is rather interesting to find that the surgeons of this time tried to obliterate the canal by means of the cautery, or inflammation-producing agents—arsenic and the like—a practice that recalls some methods still used more or less irregularly. They also used gold wire as a support; it was to be left in the tissues, and was supposed to protect and strengthen the closure of the ring. At this time all these operations for the radical cure of hernia involved the sacrifice of the testicle, because the old surgeons wanted to obliterate the ring completely, and thought this the easiest way. Chauliac criticizes the operation in this respect, but says that he has “seen many cases in which men possessed of but one testicle have procreated, and this is a problem where the lesser of two evils is to be chosen.”
While he discussed hernia operations so freely, the great French surgeon did not believe that everyone who suffered from a hernia ought to be submitted to an operation. He quite agreed with Mondeville who, in the preceding generation, declared that many operations for hernia were done not for the benefit of the patient but for the benefit of the surgeon—a mode of expression that is likely to strike a sympathetic chord in some physicians’ minds even at the present time. Chauliac’s rule was that no operation should be attempted unless the patient’s life was put in danger by the hernia, but that a truss should be worn to retain it. He emphasized that trusses should not be made according to rule, but must be adapted to each individual, and he invented several forms of trusses himself. He developed the method of taxis by which hernias might be reduced, suggested an exaggerated Trendelenburg position for operations for hernia and for the manipulations necessary for the reduction of hernia.
The technique of some of these old surgeons is a never-ending source for surprise. The exaggerated Trendelenburg position in the operation for the radical cure of hernia—the patient being fastened on an inclined board, head down, so that the intestines would fall away from the site of operation—was used by Guy de Chauliac, who probably obtained a hint of it from Italy. He also employed extension in the treatment of fracture of the thigh, inventing an apparatus by which this might be continued for a long time until the muscles were relaxed from overtiredness. He made use for this purpose of a weight suspended on a cord which ran over rollers. He also adapted stiffened bandages of various kinds, especially employing white of egg for this, and sometimes moulding bandages to the limbs in cases of fracture. Yperman, the Flemish surgeon of this time, knew and used the œsophagus tube for artificial feeding, and a number of various kinds of instruments were invented for the urethra, including bougies of wax, tin, and silver. In diseases of the bladder and in gonorrhœa John Ardern employed astringent injections.
Probably what ought to be considered the most important work of the French surgeons of the Middle Ages has been quite misunderstood until recent years. In his paper on “The Origin of Syphilis,” at the Seventeenth International Congress of Medicine (London, 1913), Professor Karl Südhoff of Leipzig (see Transactions) reviewed the use of mercury in the form of mercurial ointment during the later Middle Ages, and the reputation that it had acquired for the cure of ulcers, skin eruptions of various kinds, and other distinctly objective lesions. It is perfectly clear now that the success of this form of therapy was due to the fact that syphilis was being treated. The French surgeons of the South of France developed the empiric discovery of the value of this remedy, the first hint of which had probably come to them from the Italians. It is one of the few specifics in the history of medicine. Needless to say, it is still with us, and still the accepted medication in spite, as Professor Südhoff notes, of the often-attempted replacement of it down the centuries by some form or other of arsenic treatment, though this has always been afterwards abandoned, and it would seem as though our generation might furnish another instance of the triumph of the medieval mercurial treatment over arsenic.
The real reason then, it would seem, why syphilis came to be called the morbus Gallicus, or French Disease, was because when knowledge of its differential diagnosis was generalized, physicians at the same time learned of the remedy which could be so successfully employed for its treatment, the value of which had been determined as the result of the careful observations of the surgeons of South France. It is probable, as I have said, that the original idea for this form of treatment came from the Italian surgical traditions brought over from Italy by Lanfranc and his contemporaries at the end of the thirteenth century. There can be no doubt at all, however, of the power of clinical observation of the medieval surgeons who gave us this wonderful advance in therapeutics.
The most distinguished pupil of Guy de Chauliac was Pietro d’Argelata, who died about 1423 as a professor at Bologna, but whose textbook, “The Cirurgia,” was among the first of medical books to be printed at Venice in 1480. His teaching was still a living force at that time, and it is evident that he had attracted wide attention in his own generation. He taught the dry treatment of wounds, suggesting various powders to be employed on them, and gave his experience with sutures and drainage tubes in wounds.
Ligatures are often supposed to have been invented much later. They have been attributed to Ambroise Paré and other surgeons of the Renaissance period, but were probably used at many times during the Middle Ages, and had been invented and frequently employed by the Greeks. They invariably went out of use after a time, however, and had to be reinvented. As I said in “Old-Time Makers of Medicine”:
“It is hard to understand how so useful an auxiliary to the surgeon as the ligature—it seems indispensable to us—could possibly be allowed to go out of use and even be forgotten. It will not be difficult, however, for anyone who recalls the conditions that obtained in old-time surgery to understand the succession of events. The ligature is a most satisfying immediate resource in stopping bleeding from an artery, but a septic ligature inevitably causes suppuration, and almost inevitably leads to secondary hæmorrhage. In the old days of septic surgery, secondary hæmorrhage was the surgeon’s greatest and most dreaded bane. Some time from the fifth to the ninth day a septic ligature came away under conditions such that inflammatory disturbance had prevented sealing of the vessel. If the vessel was large, the hæmorrhage was fast and furious, and the patient died in a few minutes. After a surgeon had had a few deaths of this kind he dreaded the ligature.
“Eventually he abandoned its use, and took kindly even to such methods as the actual cautery, red-hot knives for amputations and the like, that would sear the surfaces of tissues, and the bloodvessels, and not give rise to secondary hæmorrhage. A little later, however, someone not familiar with the secondary risks would reinvent the ligature. If he were cleanly in his methods, and, above all, if he were doing his work in a new hospital, the ligature worked very well for a while. If not, it soon fell into innocuous desuetude again. In any case, it was only a question of time until it would be abandoned.”
There was at least one, and probably a number of English surgeons who were doing excellent work in the latter part of the Middle Ages, but John of Ardern wrote a book which has come down to us, and from him we may judge the character of his contemporaries. He was educated at Montpellier, and practised surgery for a time in France. About the middle of the fourteenth century, according to Pagel, he went back to his native land and settled for some twenty years at Newark in Nottinghamshire; and for nearly thirty years longer, until near the end of the century, practised in London. Ardern’s speciality was diseases of the rectum, but he made special studies in the treatment of fistulas everywhere in the body. He was an expert operator, and seems to have had excellent success in this field. He made careful statistics of his cases, and was quite as proud as any modern surgeon of the large numbers that he had operated on, which he gives very exactly. He was the inventor of some new instruments and of a clyster apparatus. We know something also about his fees, and there is no doubt that he obtained quite as good fees in proportion to the value of money as even any specialist of the modern time.
Ardern gives many evidences of his power of clinical observation, and incidentally makes it very clear that the eyes of the men of his time were not so held from seeing the things that lay before them as is often assumed. Mr. D’Arcy Power, in the paper on “The Lesser Writings of John Ardern” which he read before the section on the History of Medicine at the Seventeenth International Congress (see Transactions), has quoted a series of paragraphs from Ardern which make it very clear how accurate an observer this fourteenth-century Englishman was. Here, for instance, is his description of epidemic sore throat in his time, probably diphtheria, for the death within five days through strangling would seem to point to this:
“And note diligently that in the sqwynancy [quinsy] and in all the swellynges of the throte and the nekke and in all the lettynges and swolowynge as whanne the pacient thereof is oftetymys dysposyd to the deeth withinne schort time and I have seye manye deyed thereof within v dayes thorough stranglynge. To the weche it is to know that ther is nothynge more profytablere therefore thane to use glysteryes of malowys, mercurye [cheno-podium?] branne and oyle or buttre, hony and Sal gemme or comone salt. This operacione draweth the wykkyd humours to the inner partyes that causeth the syknesse and so it helpeth the sqwynnancye.”
Ardern’s description of rabies, its fatality, and of how a mad dog acts, exemplifies still further his accuracy of clinical observation. Only one who had seen many cases and understood them, and had had many mad dogs under observation, could have given the details he does. A single paragraph confirms the idea that the medieval surgeons had very clearly recognized the disease, and knew as much about it as was known until our own generation added something of more definite knowledge of the affection than could be gained by mere clinical observation. Ardern says:
“The bytynge of a wood [mad] dogge is more venemous and perilous thane it is of a serpente, ffor the venyme of a wood dogge ys hydd often tymes by the hole yere togydere and other whyle by the ii [two] yere and after some auctours it wole endure vii yere or it sle [slay] a man. And note wheyther it be longe tyme hydd or schorte or that it slee ther comene tofore to the pacient thes tokenys medlynge and chaungynge of wytte and resone and abhominacione and lothsomnesse of cold water that is clene and pure. And whane suche sygnys fallen to him that is byten of a wood hound schall unnethe or ellys [seldom or never] escape it.
“The tokenys of a wood dogge ben these; the furste is he knoweth not his lord ne his mayster and he falleth into a voyd goyinge allone with boowynge of his heed and hangynge of the erys [ears] as other wyse than ne he hadde hemin his helthe and the yene [eyes] of him ben rede and the fome cometh out at the mowth and he wole berke at his oune schadowe and he hath ane hos [hoarse] berkynge, and other houndes fleene from hyme and berken towardys hyme. And yf a schyvere [slice] of breed be folden or wette in the bytynge of the sore and yoven a dogge to ete, yf that he ete it, it is a token that the dogge is not wood, for and the dogge be wood tha other dogge that the breed is yoven to wole not ete it, but that he be over moche hungry, and yf he denye to ete the seyde breed, out-take [unless on] the condicione aforeseyd, thane is the dogge wood.”
Ardern’s description of a case of traumatic tetanus is very interesting, because it contains so many elements that are familiar in the history of this affection. The fact that it occurred in a gardener from a hook, so likely to be infected with tetanus bacilli from hay or grass, and that the wound was made where the thumb joins the hand and where, as we know now, the construction of the tissues is so favourable to that burying of the tetanus bacilli away from the free oxygen of the air, giving it a chance to grow anaerobically, all show the disease exactly as in our own time. The other details of the case probably indicate a wound of an important bloodvessel, secondary hæmorrhage after suppuration had been established, and then the development of fatal subacute tetanus.
“A gardinere whyle that he wrowghte in the vynes kytte his owne hande with ane hooke uppone a ffryday after the ffeste of Seynt Thomas of Caunterbury in somere so that the thoombe was altogydere departyd from the hande saff only in the juncture that was joyned to the hande, and he myghte boowe bakward the thoombe to his arme and ther stremyd out therof moche blood.
“And so touchynge to the cure. The thoombe was furst reduced in to his furste ordre and sowyd and the blood was restreyned with the reed pouder of launfrankes [Lanfranc’s red powder] and with the heerys [hairs] of ane hare and it was not remevyd une-to the iiide day when it was remevyd tther apperyd no blood. Thanne was ther putte therto tho medicines that engendren blood, every day ones repeyrynge the wounde, and tho it begane to purge itselffe and to gadere mater. And in the iiiithe nyght after the blood brak out abowte mydnyght in the wheyghte of ii poundes. And whane the blod was restreyned the wounde was repeyred frome day to day as it was furste.
“Also in the xithe nyght abowte the forseyd oure the blood brake owt ayene [again] in more quantyte thane it dyde afore tyme, nevertheless the blood was staunched, and by the morne the pacient was so taken with the crampe in the chekes [cheeks] and in the arme that he myght resseyve no mete in-to his mowth ne neyther opene the mowyth (lockjaw) and so vexynge the pacient in the xv day the blood brake out ayene owt of mesure and alwey the crampe endured forth and in the xx day he dyde.”
Another important surgeon of the West of Europe whose book has come down to us was John Yperman, who owes his name to the fact that he was a native of the town of Ypres (in Flemish Ypern) in Flanders. Yperman was sent by his fellow-townsmen to Paris in order to study surgery, apparently at the expense of the municipality, because they wanted to have a good surgeon in their town, and Paris seemed the best school at that time. Ypres, so familiar now as the scene of bloody battles, had become even before the war one of the less important cities even of Belgium, with less than 20,000 people. It was in the thirteenth century one of the greatest commercial cities of Europe, and probably had several hundred thousand inhabitants. The great hall of the Cloth Guild, one of the architectural triumphs of the time, and such an attraction for visitors to the town ever since (destroyed in the war) was built at this time, and is another tribute to the community feeling of the citizens, who determined upon the very sensible procedure of assuring the best possible surgery for themselves and fellow-citizens by having one of their townsmen specially educated for that purpose. Yperman’s book on surgery was well known in his own time, but remained unprinted until about half a century ago (1854), when Carolus of Ghent issued an edition. Subsequent editions were issued by Broeckx, the Belgian historian (Antwerp, 1863), and by van Leersum (1913), who gathered some details of the great Flemish surgeon’s life. After his return from Paris, Yperman obtained great renown, which maintains in the custom extant in that part of the country even yet of calling an expert surgeon “an Yperman.” He is the author of two works in Flemish. One of these is a smaller compendium of internal medicine, which is very interesting, however, because it shows the many subjects that were occupying physicians’ minds at that time. He treats of dropsy, rheumatism, under which occur the terms coryza and catarrh (the flowing diseases), icterus, phthisis (he calls the tuberculous, tysiken), apoplexy, epilepsy, frenzy, lethargy, fallen palate, cough, shortness of breath, lung abscess, hæmorrhage, blood-spitting, liver abscess, hardening of the spleen, affections of the kidney, bloody urine, diabetes, incontinence of urine, dysuria, strangury, gonorrhœa, and involuntary seminal emissions—all these terms are quoted directly from Pagel’s account of his work.
There is not much to be said of the surgery of Germany during the Middle Ages, though toward the end of this period a series of important documents for the history of surgery were written which serve to show how much was being accomplished, though the subsequent religious and political disturbances in Germany doubtless led to the destruction of many other documents that would have supplied valuable information. Heinrich von Pfolspeundt’s book, which is a work on bandaging—“Bundth-Ertzney”—was published in 1460, and the experience for it was therefore all obtained in the Middle Ages. While its main purpose is bandaging, it contains many hints of the surgical knowledge of the time. There are chapters devoted to injuries and wounds, though it is distinctly stated that the book is for “wound physicians” (Wund Aertzte) and not for cutting physicians (Schneide Aertzte)—that is, for those who do operations apart from wounds. There are two operations described, however, that have particular interest. One of them involves the plastic surgery of the nose, and the other the repair of a hare-lip.
Pfolspeundt suggested that stitches should be placed on the mucous surface as well as on the skin surface, after the edges of the cleft in hare-lip had been freshened in order to be brought closely together for healing with as little deformity as possible. Perhaps his most interesting surgical hint for us is a description of a silver tube with flanges to be inserted in the intestines whenever there were large wounds, or when the intestines had been divided. The ends of the gut were brought together carefully over the tube and stitched together, the tube being allowed to remain in situ. Pfolspeundt says that he had often seen these tubes used and the patient live for many years afterwards. While this resembles some of the mechanical aids to surgery of the intestines that have been suggested in our time, this was not the first mechanical device of this kind that had been thought of. One of the later medieval surgeons in Italy, one of the Brancas, had employed the trachea of an animal as the tube over which the wounded intestines were brought together. This had the advantage of not having to be passed, for after a time it became disintegrated in the secretions, but it remained intact until after thorough agglutination of the intestines had occurred.
Larger Image
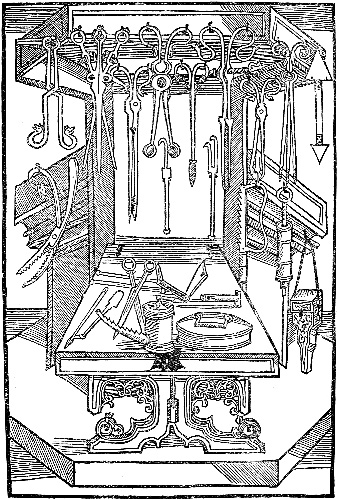
BRUNSCHWIG’S SURGICAL ARMAMENTARIUM
From Gurlt’s “Geschichte der Chirurgie”
Hans von Gerssdorff and Hieronymus Brunschwig, who flourished in the latter half of the fifteenth century in Germany, have both left early printed treatises on Surgery which give excellent woodcuts showing pictures of instruments, operations, and costumes, at the end of the medieval period.
CHAPTER VIII
ORAL SURGERY AND THE MINOR SURGICAL SPECIALITIES
The surgical specialities, as they are called—that is, the surgery of the mouth, throat, and nose, and of the eye and ear, as well of course as of certain other portions of the body—have developed to a striking extent in our time. As a consequence of this recent development, there is an impression prevalent that this is the first time that serious attention has been paid by surgeons to these phases of their work. The feeling is probably that the minor operations usually required in the surgical specialities were either thought so trivial, or involved such delicate technique, that they never received due attention, rather than that they were deliberately neglected.
Because of this very general persuasion, even among physicians, it is all the more interesting to trace the phases of attention during the Middle Ages to these special subjects in surgery, which was far from lacking at any time, and which led at various periods to some rather important developments. While specialism is considered new by most people, it must not be forgotten that at every time in the world’s history, when men have had much chance to think about themselves rather than the actual necessities of the situation in which they were placed, and the things they were compelled to do for actual self-preservation, specialism has enjoyed a period of more or less intense evolution. It is rather easy to trace this in the Ebers Papyrus near the beginning of the second millennium b.c.; and Herodotus called attention to the fact that the old Egyptians had divided the practice of medicine into many specialities. His passage on the subject is well known.11