 полная версия
полная версияPsychotherapy
Nearly all of them when carefully questioned prove to have special foods that are more difficult of deglutition than others. Not infrequently these idiosyncrasies for food are found to follow ideas with regard to their digestibility. If the patient is hurrying for any reason and suddenly becomes conscious that he is not masticating sufficiently, swallowing at once becomes much more difficult.
The main element in the treatment, however, must be as far as possible to get the patient's mind off his condition. The more attention he gives to it the worse it will be. No treatment that we have will cure it any more than stuttering can be cured, though a deliberate effort to form a habit for the control of the swallowing muscles will often do much to lessen the discomfort and the inability to swallow.
It is important in all these cases to be sure that there has been no incident in childhood which might have caused the production of scar tissue in the esophagus with a consequent stricture. Sometimes it is many years before this manifests itself and, as in the case of the urethra, even ten to twenty years may pass before serious trouble comes. When the first symptoms are noticed, the actual stricture may be so slight as scarcely to be possible of diagnosis by the bougie. Occasionally the first symptom of a cancer of the esophagus is an inability to swallow, and cancers of the esophagus have been known to occur in quite young people, especially young men. I remember seeing a case at autopsy in Vienna where the first symptom had been the difficulty of swallowing and the man, at the recommendation of friends, swallowed a glass of beer with some black peppers in it and these stuck in his esophagus and produced death. Such cases are exceptional but must not be forgotten. Neurotic esophageal stricture is entirely benignant and its prognosis altogether favorable.
Treatment.—The treatment of stuttering presents the best example that we have of the influence of the mind over neurotic difficulties of any and every kind. Many forms of treatment have been announced as successful, most frequently in the hands of men who have themselves been stutterers and who have helped themselves by them. This would seem to make it clear beyond all doubt that discoveries in direct therapeutics had been found. As a matter of fact, however, when a review of all the methods is made, they are seen to be so different from one another and founded on such essentially diverse principles that the only common connecting link to be found is in the occupation of mind with something else besides speech which all these methods recommend. We have had successful cures announced by surgery, by discipline, by making speech more difficult by obstacles of various kinds, by special positions of the tongue—up against the palate or down against the floor of the mouth—by associated movements, by rhythmic speech, by special control of the muscles of respiration, and of many other structures much less related to speech. The interesting phase of all this is the uniform success claimed by different specialists using many different methods.
From the beginning of history cures have been suggested. That idea, still held among the non-medical, that the sufferer from a difficulty of speech is tongue-tied and needs to have the frenum cut, is as old as the history of medicine. Galen suggested cauterization of the tongue. Aetius, the first prominent Christian physician of whom we have any record, divided the frenum of the tongue. So did Paul of AEgina. Of course, in the Renaissance, when the old medical classics were revived, this became a favorite method of treatment. Hildanus is sure that it accomplishes great things. This idea has never been entirely given up, and recurs from time to time in the practice of those who do not reason much, but who look for some ready explanation and, above all, some direct method of treatment. Much more serious surgical intervention has been suggested from time to time, however. Velpeau advised division of the extensor muscles of the tongue. Of course a number of surgeons have quite properly insisted on the removal of the tonsils, uvula, polyps in the nose and other obstructions of respiration.
Singing in Treatment .—A number of the stuttering cures employ singing as a method of training in forthright utterance. Few people stutter when they sing. Most people can be given confidence in themselves and their power to talk right on by being shown that as soon as they try to follow a set of notes there is little or no difficulty in utterance. The teaching of singing, then, is of distinct value in many cases. Taking advantage of this a number of those who correct stuttering endeavor to introduce a certain rhythm into speech. So long as the rhythm can be maintained stuttering does not occur. As Kussmaul has pointed out the rhythmus acts as an efficient will-regulator, so that nerve impulses go down regularly and are not interrupted by consciousness and by the sudden starts and stoppages due to fear and tremor and mental uneasiness. Undoubtedly the lesson of this method of teaching is extremely important as an index of how stuttering may be relieved.
Regulation of Respiration .—A number of systems to correct stuttering depend on the regulation of breathing. It has been shown over and over again, and notably by Prof. Gutzman of Berlin,41 that one of the most important differences between stutterers and those who talk naturally is that the normal individual talks during expiration as may be seen in Fig. 23, while the stutterer begins at the end of inspiration or at least where normally on the respiratory curve expiration is just about to begin, but instead of permitting his diaphragm to go up as in ordinary expiration, the stutterer makes it sink lower and lower in a forced inspiration.
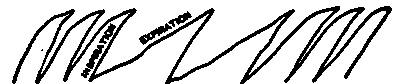
Fig. 23.—Normal Diaphragm Curve in Normal Breathing. Expiration as we Talk Normally.
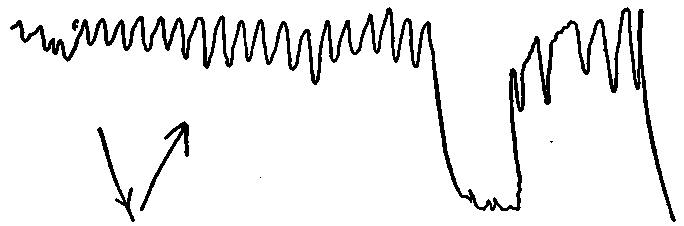
Fig. 24.—Curve in Diaphragm Before and During Talking by a Stutterer.
Attention to Something Besides Speech .—The attention must be centered on something besides speech itself. This is the important element in any method of treating stuttering. If it is allowed to occupy itself with that nothing will save the individual from getting tangled in the efforts that he makes to co-ordinate the complex movements necessary, though if he would only allow them to proceed automatically, as do the rest of mankind, there would be no difficulty at all. Washington Irving, so ready with the pen, could not utter two successive sentences at a banquet without having to sit down, with expression absolutely inhibited from excitement. Expression, thought, utterance—all may be inhibited by overconscious attention, which may also disturb all other complex activities.
The most interesting methods of treatment for stuttering are those which involve the use of various hindrances to speech and which would seem to be least likely to make it possible for a person already laboring under speech difficulties to talk with more ease. The secret is, of course, that the added impediments so distract the attention of the patient that he is unconscious of the co-ordination necessary for speech and so accomplishes it without difficulty. It is because of over-attention to himself that the disturbance occurs. These methods developed very early in history. We all know the tradition of Demosthenes overcoming his impediment by placing pebbles in his mouth. One of the most earnest advocates of a similar method, who had himself suffered very seriously from stuttering was the Rev. Charles Kingsley, one of the most distinguished of English literary men. He cured himself, or at least greatly relieved his symptoms, by keeping a cork fast between his back teeth.
There have been many other curious suggestions for the cure of stuttering. What was known as the American method had great vogue in the early part of the nineteenth century. It was probably invented by Yeats of New York, though it came to be known as the Leigh method. Yeats, himself a physician, seemed to fear that he might fall into professional disrepute if he advertised the method in any way, so he had his daughter's governess, a Mrs. Leigh, open an institute for the cure of stuttering in which this method was practiced and it proved to be very successful. The entire secret of it was to have the patient raise the tip of the tongue to the palate and hold it there while speaking.
Another mode of treatment that attracted considerable attention consisted mainly of just exactly the opposite maneuver, that is, keeping the tongue as far as possible firmly placed on the floor of the mouth during speech. It is evident that neither of these suggestions does anything more than occupy the patient's attention with an additional activity, so that his speech function may be allowed to proceed automatically of itself, as it will if not disturbed by attention to it and by conscious attempts to regulate the various activities of it. Instruments were invented to help the patients to secure various positions of the tongue. Itard, for instance, during the second decade of the nineteenth century invented a golden or ivory fork to be placed beneath the tongue, so as to support it.
After the various methods of managing the tongue, the most popular curative maneuver has been that of regulating the breathing. During the nineteenth century there were at least a dozen different methods, all of which had a number of reported successes, of treating stuttering by means of breathing exercises.
Very simple methods of diverting the attention from speech are quite sufficient in many cases to bring improvement. For instance, the insertion of extra letters that are themselves easy to say between words or preceding consonants that are hard to utter has been a favorite method among the specialists in stuttering. Johann Müller, as I said, suggested an e. Others have suggested an n. Occasionally stutterers themselves form the habit of using an m or a to and find that it aids their facility in uttering difficult sounds over which they would otherwise halt and stutter. A combination of these methods, as, for instance, an e between all words and the placing of an easy n before the most difficult sounds, has been repeatedly revived as an infallible method of treatment.
All this serves to show that in patients whose functions are being interfered with by over-attention diversion of mind must be the main remedy. If this can be secured, the function they are disturbing will be allowed to proceed unhampered. What will prove effective for one patient will fail with another, however. After the patient gets used to a particular form of diversion another must be tried. Simple methods are sometimes sufficient to secure good results. The one thing is not to be discouraged and to proceed from one effort to another, satisfied even if relief is obtained for a while, for after relapse another method of treatment may always be tried.
Suggestion for Stuttering .—There are many systems to train people out of the spasmodic inco-ordination that constitutes stuttering. All of these systems have their successes, but, as is well known, all of them have their failures. When the patient has confidence in the teacher and his method there is practically always quite a remarkable improvement, at the beginning. This improvement is more noticeable during the first month than at any other time. Not infrequently after this there is a tendency for patients to drop back into old habits, apparently discouraged, as a consequence of loss of confidence. It is the mental element that means more than anything else. It is the old, old story that we have to repeat with regard to every chronic ailment.
Distraction of Mind .—Each inventor is sure that his method is the best and his "cured cases" support his claim. Others who try his method, however, never succeed as well as he does and those who are interested invent methods of their own. I have on my desk, as I write, six different, infallible—to their authors—methods of treating stuttering. I am sure that none of them succeed absolutely, that is, none of them will cure every case and most of them will not succeed beyond a moderate degree, except where the enthusiasm and the confidence of the inventor or an immediate disciple of his is behind them to make them efficient. There are all sorts of elements in these cures, but most of them depend on their power to distract the patient from his over-attention to himself and what he is doing when he talks, so as to permit without hindrance the automatic movements which are so necessary for the complex function we call speech. Those who have spent most time in treating stutterers confess that the effect produced upon the patient's mind is an extremely important part of the treatment and that, if this cannot be secured, failure is almost certain. If the patient has no confidence that he can be cured and by this particular method, failure is inevitable from the very beginning and just as soon as a patient loses confidence improvement ceases.
CHAPTER V
TREMORS
Two types of tremors come to us for treatment: those that are quite involuntary and occur when muscles are at rest, and those that are associated with voluntary movements. The most common type of involuntary tremor is that seen in paralysis agitans to which a special chapter is devoted. After this, though coming for treatment much less frequently, is senile tremor which may, however, also be increased by voluntary movement. The tremors associated with voluntary movements are spoken of as intentional tremors. They may occur as the result of organic disease of the nervous system and the most characteristic type is that seen in multiple sclerosis. They are more frequent, however, with functional diseases of the nervous system and with emotional disturbances of various kinds. They are especially frequent as the result of dreads. Usually the idea of tremor is associated only with the head and the hands. Tremors may occur in other parts of the body, however, and tremors of the legs are particularly important. A familiar type is the tremor and unsteadiness of the legs which occur as a consequence of the dread of heights when a person unused to such situation attempts to walk across a narrow path a great distance above the ground.
Senile Tremor.—The most common of the involuntary tremors is that associated with old age. It develops in practically all very old people, but it comes to some who are comparatively young. Its occurrence at the age of fifty-five usually gives the sufferer a severe shock which is emphasized by the attitude of mind of friends toward the affection. They seem to be always sure that it is the index of rapidly advancing age and that it is practically a signal of approaching dissolution. As a matter of fact, when unassociated with gross pathological lesions, the senile tremor has no such significance. When associated with definite lesions it is the prognosis of the special condition and not any supposed significance of this particular symptom of tremor that expresses the genuine outlook in the case. Many people who live to a very old age develop tremor before they are threescore. Most of those who live to be eighty or more have some tremor that develops about or just after the age of seventy.
Significance .—Senile tremor is supposed to be due to, and in most cases probably is the result of, an overgrowth of connective tissue in the central nervous system which disturbs the ordinary conduction of nerve impulses, rendering them wavering and uncertain. This seems to indicate that it will not be long before the advancement of this sclerotic process will make serious inroads on the vigor of the individual. As a matter of repeated observation, however, the ordinary involuntary tremor of old people may last twenty years.
Reassurance .—The main principle in the treatment of tremors of the old is to make the patients realize that the symptom has no such bad prognosis as is usually attributed to it. Of course, they will find this out for themselves after a few years, but what they need is assurance at the beginning lest during the period of depression consequent upon the conclusion that the end is not far off, which seems to be forced on them by their fears and the foolish sympathy of friends, their resistive vitality should be so lowered as to permit the invasion of some serious disease. In spite of apprehensions on the part of themselves and friends, tremor is rather a good sign than a bad one. It indicates the formation of connective tissue in the central nervous system, but this is always a slow process and is usually quite benign. As a matter of fact, most sclerotic processes are so chronic as to be compensatory in their action for many other degenerations. Those in whom tremor develops early often seem to be better protected against rupture of cerebral arteries, as if the growth of connective tissue was a conservative process here also. Information of this kind helps patients not to borrow trouble because of their condition.
Intention Tremors.—The tremors that occur in association with voluntary movements are often very troublesome and may be difficult to manage. The worst cases are entirely functional. They are typical neuroses and often develop as a consequence of some serious crisis through which the nervous system has passed. In older people they sometimes pass over into paralysis agitans or a close simulant of that affection. The incident of the Texas sheriff and the Indian related in the chapter on Paralysis Agitans illustrates how these tremors may be induced.
Tremors from Fright .—Frequently the tremors have no direct connection with any action, though they may be the result of fright. A little girl bitten by a dog and much shocked may, for some time afterwards, be quite unable to stand when she sees a dog on the street, so disturbing is the tremor that comes over her. Tremors of the same kind have been connected with horses after the patient had been run down in the street, and, in one case that I saw even when the patient was only thrown out of a carriage during a runaway. Occasionally fright by a burglar may cause a distinct tremulousness that supervenes whenever the patient thereafter is wakened suddenly at night.
Influence of Dread.—Tremors of all kinds can be made worse by the dread of them. In the chapter on Dreads we discuss the disturbance of function by dreads and especially the tendency to exaggeration of pathological conditions of any kind when the patient's mind becomes concentrated on it. Steadiness in any position is due to a nice balancing of extensor and flexor muscles requiring the sending down of a continuous stream of impulses. The equilibrium is attained and maintained in spite of the fact that, as a rule, the flexor muscles are stronger than the extensors and better situated to exert their mechanical force. If anything happens to disturb this balance even to a slight degree, the mind becomes attracted to it and there is a corresponding result as in stuttering, or other complex function when surveillance is too great. It is important to remember this at the beginning of all cases of tremor, for the patient nearly always exaggerates his tremor by attention to it and can be made so much better by reassurance and diversion of mind that he is much encouraged and his general health usually improves, making him feel, even though his affection is organic, that he is being cured.
Tremors may occur in connection with almost any set of actions requiring special co-ordination of muscles, but they are especially likely to occur when a feeling of dread disturbs the control over muscles. A typical example of this is noted in shaving. There are many men who cannot shave without trembling so as to cut themselves. The feeling that they have a sharp instrument in their hand with which they may cut themselves sets up the tremor. There are others who cannot shave because they dread that while using the instrument over the important organs of the neck, and especially the blood vessels, they may be tempted to cut their throats. This is, of course, purely a dread and not a tremor. Some men find both the dread and the tremor much worse at times when they are tired and worried, and can shave very well at other times. Some men can shave very well when they are not under observation, but if anyone is looking at them they tremble and cut themselves. The safety razor usually does away with these troubles, large or small, but if it should happen that by particularly inexpert use they cut themselves even with a safety razor, especially in the throat region, the old dread and tremor reassert themselves and shaving becomes almost as difficult as before.
Self-consciousness.—Almost any position or action in which a man feels himself under observation may cause one of these tremors. As a consequence this particular set of actions may become the source of so much discomfort as to produce an intense sense of fatigue. It may, indeed, become quite impossible of accomplishment. Some teachers cannot do demonstrating work on a blackboard before a large unfamiliar class, at least not without serious efforts to control themselves, though they may be facile demonstrators before a small class. I have known men, however, who practically could not do blackboard work at all because of nervousness. Their writing went all askew and very often their thoughts would not follow one another in such order as to make demonstrations possible. Sometimes they were good talkers, so long as they did not turn their backs to the class and feel the eyes of all on them. The same thing is true of such religious services as Mass in the Catholic Church, where some of the clergymen have this feeling. I know of priests who have not said Mass publicly for years and others who can only say it in a small chapel before a few people because of the intense discomfort of the fatigue caused by this state of mind.
Stage Fright .—It is not alone the hands and the arms that tremors are likely to affect, for they may also occur in the legs. A typical and familiar case is the tremor that occurs upon the first appearance before large audiences of orators or actors or clergymen. Owing to excitement, they are unable to make flexor and extensor muscles exactly balance each other and the consequence is a tremulous movement that may be complicated by some swaying. Some people never lose this in spite of long experience in public appearance. Young people may have it upon being introduced to persons of whom they think a great deal. This passes off with years, as a rule, but in some it persists, and any excitement causes tremor of the legs and swaying movements. The effort to control this is often severe and causes intense fatigue.
Any set of movements requiring even slight co-ordination of muscles may be the subject of disturbance by a tremor. Since the writing of the book on Pastoral Medicine, a text-book of medical information meant to be of assistance to clergymen,42 I have had some rather interesting tremors associated with the performance of clerical duties brought to my attention. One of these is a trembling of the legs which makes standing at a high altar almost impossible. Another troublesome tremor is that associated with the giving of communion. Most priests find no difficulty in the performance of the rite. Some of them are much worried and anxious about it, however, and develop a slight tremor. Others become so nervous in performing the ceremony that they cannot succeed in placing the Host on the tongue of the communicant without certain false movements. These may cause them to touch the lips or the cheeks of the recipient and after this has happened a few times the giving of communion becomes practically impossible for them. Occasionally the men thus affected have no other nervous symptoms and often they are very intelligent, strong-minded men.
The General Health.—Tremor patients always complain more of this symptom when they are in a run-down condition. One of them is a wealthy merchant who, when he can be persuaded to take a vacation, comes back with nearly all the manifestations of his tremor latent or, at least, well under control. Another is a broker who at the end of a long winter of excitement and worry is at his worst, but who after a vacation in the North Woods is quite well again. Slight symptoms of this kind are not unusual in teachers, especially women, though I have seen them also in men, and are much more complained of at the end of the year when the individuals are in poorer general condition than at any other time. The symptom itself is annoying because of the notice that it attracts, but their dread that it may have some serious significance, indicating the development of a progressive lesion of the central nervous system, constitutes the worst part of their ailment. When the intentional tremor is intermittent and occurs only at times of excitement, or when the patients are under observation, they can be reassured that it is merely neurotic and that no ulterior development is to be anticipated.